

 ABOVE: Two rib raising techniques
ABOVE: Two rib raising techniques
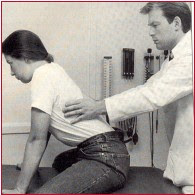
LEFT: Thoracic osteopathic lymphatic pump – hand position
When I trained as an osteopath at what is now the British College of Osteopathic Medicine
We were also taught methods and techniques that could be applied in treatment of common biomechanical problems – tennis elbow, stiff necks, back ache etc….however these were seen
to be only of relative importance in the hierarchy of what osteopaths did.
Primarily we were supposed to enhance health – and because BCOM was then named The British College of Naturopathy & Osteopathy (BCNO), we were taught that by focusing on normalising – as best possible – the framework of the body, the musculoskeletal system, we could positively influence the health of the patient.
Of course lifestyle, nutritional, stress management and psychological aspects of health enhancement were also central to the training being offered.
Indeed for many years – starting back then in the late 1950’s when I was at BCNO (graduated 1960) – my sense has been that osteopathic methods represented the structural element in total health care (with the biochemical and psychological aspects covered by the naturopathic aspects of my training).
….and so, for the past 48+ years, this is how I have practised, with osteopathy supporting the broader focus that this training gave me.
I have never believed osteopathy to be a form of musculoskeletal medicine, designed to deal with strains, sprains, joint and muscle problems, i.e. another version of physiotherapy.
And yet, that seems to be what has happened to osteopathy – which has become a virtual biomechanical repair profession, where talk of enhancing general health via osteopathy, or of actually treating people with serious health conditions, using osteopathic approaches, is frowned on by both the regulators of the profession, and those who are teaching the next generation of practitioners.
Is there any evidence that osteopathic methods can enhance general health?
You bet!
This was brought home to me when I read a 2008 paper by Hruby and Hoffman – which I heartily recommend that sceptics should read!
I will summarise a few studies that show what’s possible – and then you can decide for yourself.
1/ What evidence is there for general health benefits resulting from non-specific osteopathic methods?
Osteopaths Clark & McCombs (2006) observe that the natural post-surgical sequelae of the cumulative insults to physiology:
“are seen daily in every hospital in America: atelectasis, ileus and venous stasis (edema, deep venous thrombosis, skin ulcerations).
Allopathic medicine offers incentive spirometry, early ambulation, continuous passive motion equipment, anticoagulation drugs & skilled nursing to counteract the effects described.”They suggest that early intervention with physical (osteopathic) strategies may avert or reduce such adverse outcomes by:
1) Restoring the cranial rhythmic impulse to its full rate and excursion
2) Restoring ventilation to full capacity
3) Maintaining and/or restore peristalsis
4) Restoring the third space fluid (lymph) to circulation.
They suggest that a various techniques can be used for each of these four goals, and that some of the techniques overlap and meet multiple goals.
They base their opinion, partially on an earlier study by Sleszynski & Kelso (1993)
2/ Post operative atelectasis
A study by Sleszynski & Kelso (1993) compared osteopathic thoracic pump technique to incentive spirometry techniques, in the prevention of post-operative atelectasis.
Thoracic pump (see photograph above)was used twice daily, while spirometry was used three to four times a day.
Both treatments were effective in reducing atelectasis from a 50 percent occurrence rate to a 5 percent occurrence rate; however the manual methods achieved the result with half the number of treatments, and patients’ recovery, as measured by pulmonary function tests, occurred more rapidly.
3/ Elderly hospitalized pneumonia patients
Noll et al (1999, 2000) applied osteopathic manual methods to elderly hospitalized patients with pneumonia, with the result that the length of the hospital stay was reduced from a mean of 8.6 days, without osteopathic, to 6.6 day with osteopathic manipulative treatment (OMT). Additional benefits in this study, for those receiving OMT, included reduced length of use of intravenous antibiotics.
4/ Manual methods and pancreatitis
Radjieski et al (1998) conducted a randomized controlled study that demonstrated that in cases of pancreatitis, length of hospital stay was reduced by about one half when OMT, involving 10 to 20 minutes daily of a standardized protocol, using myofascial release, soft tissue, and strain-counterstrain techniques was given, together with standard medical care. Patients who received OMT averaged significantly fewer days in the hospital before discharge (mean reduction, 3.5 days) than control subjects
5/ Post-operative pain
Nicholas & Oleski (2002) utilised a four-step protocol composed of rib raising (see photos above), treatment of the thoracic inlet, respiratory diaphragm and pelvic diaphragm, in treatment of post-operative pain.
They report that: “Patients who receive morphine preoperatively and OMT postoperatively, tend to have less postoperative pain and require less intravenously administered morphine. In addition, OMT and relief of pain lead to decreased postoperative morbidity and mortality and increased patient satisfaction. Also, soft tissue manipulative techniques and thoracic pump techniques help to promote early ambulation and body movement.”
6/ Post-coronary bypass surgery
O-Yurvati et al (2005) documented the physiologic effects of postoperative osteopathic manipulative treatment (OMT) following a coronary artery bypass graft (CABG), to determine the effects on cardiac hemodynamics.
10 subjects undergoing CABG surgery were compared, pre-OMT versus post-OMT, measurements of thoracic impedance, mixed venous oxygen saturation and cardiac index.
Immediately following CABG surgery OMT was provided to alleviate anatomic dysfunction of the rib cage caused by median sternotomy, and to improve respiratory function.
This adjunctive treatment occurred while subjects were completely anesthetized.
Results suggested improved peripheral circulation and increased mixed venous oxygen saturation after OMT. These increases were accompanied by an improvement in cardiac index
So the evidence exists – and there is much more of the same available – not only from osteopathy, but also from chiropractic and massage therapy
Osteopaths in the UK are in danger of losing the plot, I fear – it’s a different story in the USA (where ALL of the research quoted above took place), as well as in Germany, France, and other European countries where osteopathy is rapidly expanding.
Shame!
(P
REFERENCES
Clark R McCombs T 2006 Post Operative Osteopathic Manipulative Protocol for Delivery by Students in an Allopathic Environment. American Academy Osteopathy Journal 16(20):19-21
Nicholas A Oleski S 2002 Osteopathic Manipulative Treatment for Postoperative Pain. Journal American Osteopathic Association Supplement.3:102(9):S5-S8
Noll D Shores J Bryman P et al 1999 Adjunctive osteopathic manipulative treatment in the elderly hospitalized with pneumonia: A Pilot Study .Journal American Osteopathic Association 99(3):143-152
Noll D Shores J Gamber R et al. 2000 Benefits of osteopathic manipulative treatments for hospitalized elderly patients with pneumonia. Journal American Osteopathic Association 100(12):776-782
O-Yurvati A et al 2005 Hemodynamic effects of osteopathic manipulative treatment immediately after coronary artery bypass graft surgery. 105(10):475-481
Radjieski J Lumley M Cantieri M 1998 Effect of osteopathic manipulative treatment on length of stay for pancreatitis: a randomized pilot study.Journal American Osteopathic Association 98:(5):264-272
Sleszynski S Kelso A 1993 Comparison of thoracic manipulation with incentive spirometry in preventing postoperative Atelectasis. J. American Osteopathic Association (8):834-838