
It’s well over 100 years since Bohr first described Respiratory Alkalosis – and I am constantly amazed at how few practitioners/therapists – of all professions – are aware of the clinical importance of this inevitable side-effect of the widespread habit of rapid upper-chest, breathing !
As Jensen et al (2004) note: “The dynamic binding or release of oxygen and carbon dioxide in response to the relative abundance of these components of aerobic metabolism was described by Bohr and his assistants in 1904”
- Respiratory alkalosis occurs when CO2 exhalation exceeds the rate of accumulation and pH rises (normal ± 7.4).
- Alkalosis induces vascular constriction, decreased blood flow, and inhibition of O2 transfer from haemoglobin to tissue cells (this is a key Bohr effect).
- Incompletely oxidised metabolic products (e.g., lactic and pyruvic acid) accumulate, via anaerobic energy production pathways, particularly in deconditioned individuals.
And the body fights back, as it tries to rebalance the pH by excreting bicarbonate via the kidneys – as Nixon & Andrews (1996) noted:
- Reduced CO from hyperventilation leads to alkalosis. Rebalancing occurs via the kidneys excretion of bicarbonate
- One result of this “buffering” is increased acidity due to anaerobic energy production in deconditioned individuals
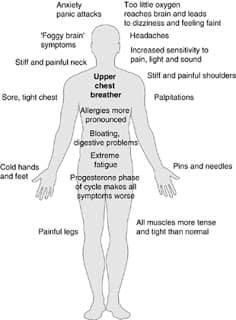
- Symptoms associated with alkalosis emerge — fatigue, brain fog, increased pain sensitivity, anxiety, and more.
The result is a catalogue of symptoms —-see the picture:
The ramifications of altered blood pH, towards the alkaline end of the spectrum, may also relate to more general features such as muscle tone, balance and motor control.
Take for example the report by Klingler et al (2005) that ‘Fibroblasts maintain the ability to become contractile by expressing smooth muscle actin stress fibers, as well as special focal adhesion on their membrane.” Contractility appears to be pH dependant, however the precise effect of respiratory alkalosis remains unclear.
- Symptoms may include circumoral numbness and carpal spasm
- Respiratory alkalosis secondary to hyperventilation is probably the most common cause of acute ionised hypocalcaemia.
- Binding between calcium and protein is enhanced when serum pH increases, resulting in decreased ionised calcium (Bansal & Hooda 2013 )
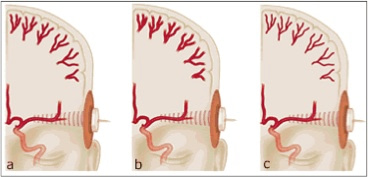
- Cerebral vasoconstrictive & vasodilating effects of hypocapnia and hypercapnia were observed (Van den Bergh et al 2013)……. O2 availability in the brain is reduced by 40% as a result of about a minute of over-breathing (HVS). In addition, glucose critical to brain functioning is markedly reduced as a result of cerebral vasoconstriction (Curley et al 2010)
Signs and Symptoms of Respiratory Alkalosis
Central Nervous System Symptoms
- Lightheadedness
- Vertigo
- Confusion
- Headache
- Tinnitus
- Blurred vision
- Syncope
Peripheral Nervous System Symptoms
- Circumoral/limb paresthesias
- Cramps
- Tremor
CNS Signs
- Ataxia
- Chvostek’s sign
- Tremor
- Encephalopathy
- Coma
- Seizure manifestations
PNS Signs
- Myoclonus
- Tetany
I have written about these issues many times…as these articles/blog postings illustrate:
https://leonchaitow.com/2008/01/31/breathing-patterns-connective-tissue-and-soft-shelled-eggs/
https://leonchaitow.com/2005/12/14/understanding-and-rehabilitating-unbalanced-breathing/
https://leonchaitow.com/2010/02/14/breathing-and-bodymind-balance/
,….and as this book explores:
http://astore.amazon.co.uk/leonchaitow-21/detail/0702049808
http://astore.amazon.com/leonchaitowco-20/detail/0702049808

References
- Bansal T Hooda S 2013 Hyperventilation causing symptomatic hypocalcaemia during labour in a parturient. Egyptian Journal of Anaesthesia 4(29):333-335
- Curley G et al 2010 Hypocapnia and the injured brain: More harm than benefit. Critical Care Medicine 38(5):1348-1359
- Jensen F 2004 Red blood cell pH, the Bohr effect, and other oxygenation-linked phenomena in blood O2 and CO2 transport Acta Physiologica Scandinavica 182(3):215-227
- Klinger W et al 2005 Active fascial contractility. Medical Hypotheses. 65(2):273–277
- Nixon P, Andrews J. 1996 A study of anaerobic threshold in chronic fatigue syndrome (CFS). Biol Psychol. 43:264
- Van den Bergh O et al 2013 Anxiety, pCO2 and cerebral blood flow. Int. Jnl Psychophysiology 89 :72–77