

Chronic pelvic pain (CPP) and dysfunction is widespread.
Much of the distress of CPP and its frequently associated symptoms – which may be as varied as interstitial cystitis, stress incontinence and dyspareunia – is amenable to manual therapy interventions.
While there are numerous possible causes and aggravating factors, excessive tone in pelvic floor muscles is a frequently observed feature.
Fitzgerald et al (2009) note that:
“The etiology of the somatic abnormalities in patients with urological pain syndromes is not known.
It is possible that the somatic abnormalities found in the lumbosacral dermatomyotomes in patients with IC/PBS are secondary, ie referred from a primary pelvic visceral abnormality.
It is equally possible that these somatic abnormalities are a primary phenomenon and may themselves give rise to secondary visceral hypersensitivity. The latter possibility is supported by recent animal studies demonstrating induction of visceral (bladder) hypersensitivity by experimental injury to a somatic (sciatic) nerve that shares innervation with the viscus.
Clinically the somatic abnormalities associated with IC/PBS are obvious and have been recognized for some time.
It is appropriate that the role of the short, painful and/or hypertonic pelvic floor in the development of chronic genitourinary conditions has now begun to inform physiotherapeutic interventions aimed at rehabilitation. Whether the somatic abnormalities are primary or secondary, our studies suggest that it is clinically valuable to address and relieve them, as demonstrated …. using specialized [manual physical therapy].”
I have emphasised the ‘short-tight pelvic floor’ issue reported by Fitzgerald, since it is now generally accepted that this phenomenon is a key to much CPP – rather than weak hypotonic pelvic floor muscles.
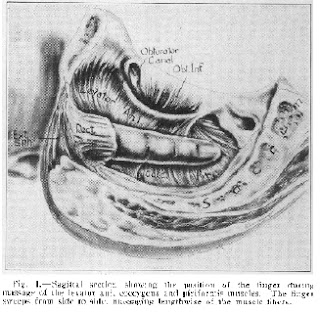
The first modern observation of this in relation to coccygeal pain was in 1859 (by Simpson), as reported in his classic paper “Coccygodynia and pain in the superior gluteal region” by Thiele (1937). Thiele developed a simple strategy for treating high-tone muscles in the pelvic floor – now named after him as Thiele Massage. See the photograph of an illustration from his paper in the Journal of the American medical Association – the legend of which states: “Sagital section showing the position of the finger during massage of the levator ani, coccygeus and piriformis muscles. The finger sweeps from side to side, massaging lengthwise of the muscle fibers.”
The method (Thiele massage) is therefore simple – a series of digital strokes of the key (reachable) pelvic floor muscles, from origin to insertion, for approximately 5 minutes – with periodic stationary periods of 10 to 15 seconds when active trigger points are identified (i.e. where pressure on them reproduces familiar symptoms – for example burning, or urgency, or radiating or distant referred pain). (Oyama et al 2004)
I have also found that it is useful to add positional release methods during such treatment – for example using pressure applied from an external pelvic contact, such as the ischial tuberosity, or the ASIS, in order to markedly modify perceived discomfort/pain for 15 to 20 seconds. Another useful addition may involve having the patient mildly isometrically contracting the tissues being compressed, for a few seconds, to promote relaxation of these.
Fitzgerald et al (2009) strongly emphasise the importance of internal and external trigger point activity in maintenance of CPP – and many associated symptoms.
Loving et al (2012) in a systematic review of evidence, urge caution in interpretation of the evidence to date: “Only small and largely non-randomised studies have been undertaken of physiotherapeutic interventions and this greatly limits the available evidence on which to base clinical practice. High quality randomised clinical trials are therefore urgently needed”
- Fitzgerald MP, Anderson RU, et al 2009 Randomized multicenter feasibility trial of myofascial
physical therapy for the treatment of urological chronic pelvic pain syndromes. J Urol 182:570–580. - Loving S et al 2012 Does evidence support physiotherapy management of adult female chronic
pelvic pain? A systematic review. Scandinavian Journal of Pain 3:70–81 - Oyama IA, Rejba A, Lukban JC et al: 2004 Modified Thiele massage as therapeutic intervention for female patients with interstitial cystitis and high-tone pelvic floor dysfunction. Urology 64: 862.
- Thiele GH: Coccygodynia and pain in the superior gluteal region. JAMA 109: 1271–1275, 1937.